How can age-related farsightedness be corrected?

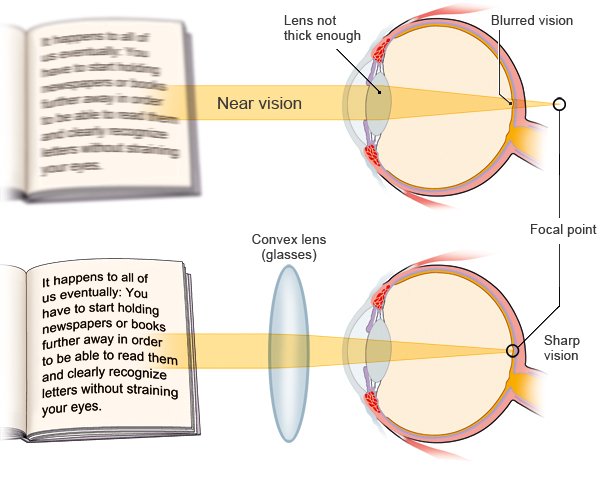
Our ability to see things close-up gets worse with age. This age-related farsightedness is known as presbyopia. Although it can’t be reversed, it is easy to correct. The simplest way is to wear reading glasses. Laser treatment and surgery have hardly any advantages, but are associated with a lot of risks.
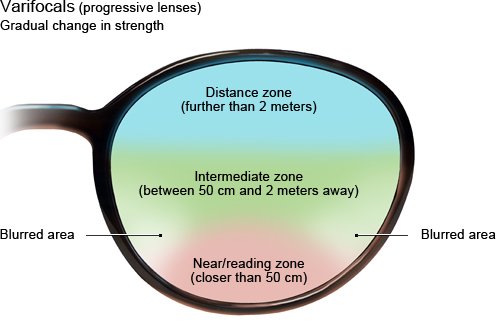
Presbyopia usually becomes noticeable in your mid-forties. At first it’s often only a problem when reading. Wearing reading glasses is then a simple and effective solution for people who don’t already have other problems with their eyesight. If you already had to wear glasses or contact lenses before, you can use glasses with varifocal or multifocal lenses to avoid having to switch between different pairs. Multifocal contact lenses are an alternative to multifocal glasses. They also allow you to see both nearby and distant objects clearly.
Laser treatment and other kinds of eye surgery are called refractive surgery. They change the eye in a way that corrects the vision problem. But many of the procedures are still being tested. The advantages of not having to wear glasses or contact lenses have to be weighed against the possible risks associated with the procedure. For instance, your spatial vision (your ability to judge how close or far away things are) may be worse afterwards, or you may suddenly have trouble seeing things that are further away. In Germany, the costs of these procedures aren’t covered by statutory health insurers.