Torn ACL: What are the pros and cons of surgery?

A torn ACL (anterior cruciate ligament) can be treated conservatively or with surgery. The advantage of conservative treatment is a faster recovery. One drawback is that the knee may not be stable enough afterwards. Because of this, about half of all people who first have conservative treatment decide to have surgery in the end after all.
The surgery involves replacing the torn ACL with a graft (tissue from your own body). A piece of tendon tissue is taken from the inner side of your thigh, the patellar tendon, or the quadriceps tendon. The tendon graft tissue is then anchored to the knee in the same position as the original ACL, using screws, buttons, or pins. Several months of rehabilitation treatment are recommended after the surgery.
In conservative treatment, the ACL is not treated with surgery. Instead, rehabilitation is started as soon as possible. The goal of rehabilitation is to strengthen the muscles that stabilize the knee so they can take over the job of the missing ACL. Sometimes parts of the torn ACL grow together with the posterior cruciate ligament, which makes the knee more stable.
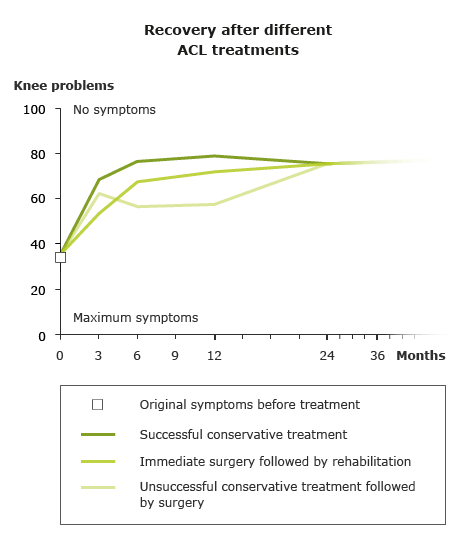
Swedish researchers did a study to examine and compare the advantages and disadvantages of the two treatment approaches.