Low-risk prostate cancer: Active surveillance or treatment?

Low-risk prostate cancer often grows very slowly, or doesn't grow at all. Because of this, a treatment approach known as “active surveillance” can be considered as an alternative to radiotherapy or surgery. In this approach, the tumor is monitored regularly and only treated with radiotherapy or surgery if it grows.
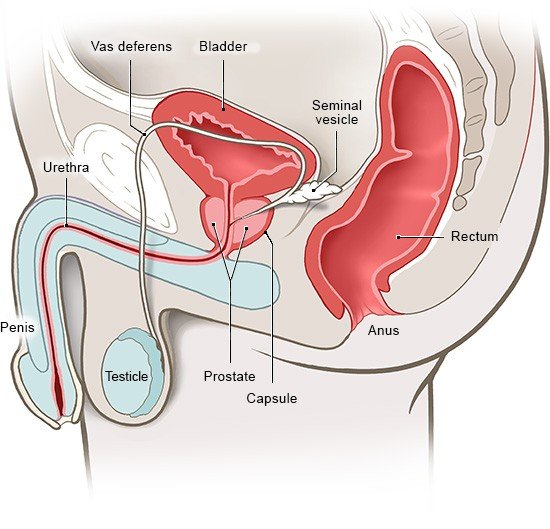
Prostate cancer is described as low-risk if it is only found in the prostate (localized) and it is highly likely to grow only very slowly, or not at all (low risk of progression). The medical criteria for low-risk prostate cancer are:
- The cancer is found in only one of the two sides (lobes) of the prostate.
- The cancer takes up less than half of the affected prostate lobe.
- The cancer cells haven’t mutated (changed) much and aren’t very aggressive.
- The cancer hasn’t spread to any lymph nodes or led to the growth of tumors (metastases) in other parts of the body.
Even if the diagnosis can be worrying: Low-risk prostate cancer grows only very slowly, or sometimes doesn't grow at all. So the chances of recovery are very good. Over a time period of 15 years, about 3 out of 100 men who have low-risk prostate cancer will die of this disease. In other words, about 97 out of 100 men will not die of prostate cancer in the 15 years after it is diagnosed.
There are different ways to deal with the cancer. All of the options have their pros and cons. So it's a good idea to get enough information and discuss the options with your doctors before making a decision.