Introduction

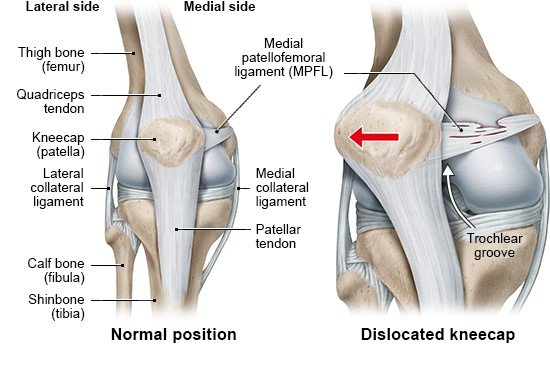
Whenever you bend or stretch your leg, the kneecap (patella) moves along a groove on your thigh bone (femur). An awkward twist of the joint or a bump from the side can knock it out of this groove. The kneecap is then “dislocated.” The medical term for this is patellar dislocation. It happens most often during sports, and is most common in teenagers and young adults.
A dislocated kneecap often moves back into the correct position on its own. But even then it’s important to have a doctor look at the knee because there could be damage to the bones, cartilage or ligaments. The kneecap is less stable after a dislocation, and it could become dislocated again.