Bayliss LE, Culliford D, Monk AP et al. The effect of patient age at intervention on risk of implant revision after total replacement of the hip or knee: a population-based cohort study. Lancet 2017; 389(10077): 1424-1430.
Beswick AD, Wylde V, Gooberman-Hill R et al. What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ Open 2012; 2(1): e000435.
Chawla H, van der List JP, Christ AB et al. Annual revision rates of partial versus total knee arthroplasty: A comparative meta-analysis. Knee 2017; 24(2): 179-190.
Deutsche Gesellschaft für Orthopädie und Orthopädische Chirurgie (DGOOC). Gonarthrose (S2k-Leitlinie, in Überarbeitung). AWMF-Registernr.: 033-004. 2018.
Falck-Ytter Y, Francis CW, Johanson NA et al. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141(2 Suppl): e278S-e325S.
Schmitt J, Lange T, Günther KP et al. Indication Criteria for Total Knee Arthroplasty in Patients with Osteoarthritis - A Multi-perspective Consensus Study. Z Orthop Unfall 2017; 155(5): 539-548.
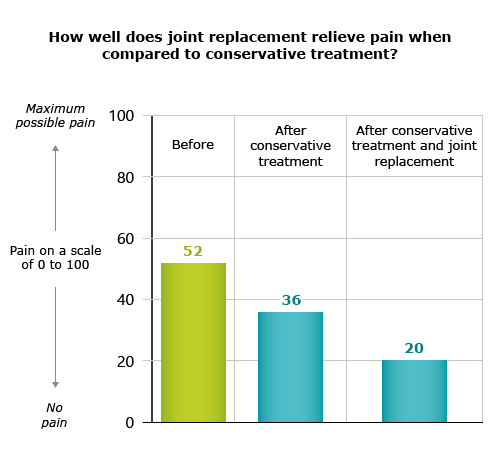
Skou ST, Roos EM, Laursen MB et al. Total knee replacement and non-surgical treatment of knee osteoarthritis: 2-year outcome from two parallel randomized controlled trials. Osteoarthritis Cartilage 2018; 26(9): 1170-1180.
Skou ST, Roos EM, Laursen MB et al. A Randomized, Controlled Trial of Total Knee Replacement. N Engl J Med 2015; 373(17): 1597-1606.
Tibbo ME, Limberg AK, Salib CG et al. Acquired Idiopathic Stiffness After Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. J Bone Joint Surg Am 2019; 101(14): 1320-1330.
IQWiG health information is written with the aim of helping people understand the advantages and disadvantages of the main treatment options and health care services.
Because IQWiG is a German institute, some of the information provided here is specific to the German health care system. The suitability of any of the described options in an individual case can be determined by talking to a doctor. informedhealth.org can provide support for talks with doctors and other medical professionals, but cannot replace them. We do not offer individual consultations.
Our information is based on the results of good-quality studies. It is written by a team of health care professionals, scientists and editors, and reviewed by external experts. You can find a detailed description of how our health information is produced and updated in our methods.